Our Perpetual Conversation
The Language of Vision & Posture
Vision may be the lead system of both the individual and the culture, but posture is its embodied and unrelenting audience. The two systems begin life developmentally far apart and quickly work to become intertwined as both the brain and body become more complex. The eyes are the bridge between the two as sight is converted to vision and posture is transformed into tone. The tapestry of this process is actually a ‘trialogue’ that anchors different dimensions of what I call our perpetual conversation. Somatics is uniquely equipped to facilitate and augment this trialogue.
Being able to shift our ‘dialect’ as we naturally transition between these ‘worlds’ is a function of this constant exchange of images and tension. Over the last 20+ years I’ve had the opportunity to learn several ‘maps’ of this subtle terrain. What I’ll be doing is pointing out highlights of what Moshe Feldenkrais called the ‘elusive obvious’. The aim is to make this hidden world more accessible and ultimately more coherent so we can better connect behavior, biology and go beyond our conditioning.
Connecting The Dots
Let’s start this by taking a ‘nickel tour’ of the developmental aspects of how these two systems create their partnership. Darryl Boyd Harmon, Ph.D, was early pioneer in this arena. He was an educator and a kinesiologist who ‘postulated the primary biological function of vision is its role in organizing spatial relationships, rather than image formation.’ 1 Here’s an overview of how and why vision and posture unify.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
The eyes are a matched pair of brightness meters. They are capable of triggering an array of real or symbolic actions in response to significant light patterns occurring within their field of awareness. Before the light patterns to which the eyes are sensitive can become accurate and meaningful sources of information about the environment, the following must occur.
- The head which houses the eyes and the neck and the body which responds to what the eyes see, must come to balance both with the light patterns and also with gravity.
- Unless the organism establishes a balanced equilibrium with the light patterns, they are likely to be inaccurately organized by the eye's receptors in the retina, and the receptors then are likely to trigger distorted neural signals.
- Therefore one of the organism's first responses to a light pattern is to turn the eyes, neck and body until there is an equal amount of light on each retina
- Coming to a balance with the light patterns simultaneously aligns the organism with gravity, thereby providing a stable base from which to respond.
- The organism's balanced equilibrium both with light and gravity results in reciprocal feedback among the eyes, neck, and trunk as each tries to equate its activity with the other.
That feedback provides the organism with the opportunity for optimal freedom to perform whatever is required to cope with the task at hand.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
That was where the cutting edge was on this topic in 1958. Here’s a more contemporary summary from a paper written in 2005. Notice how the description has changed and gotten much more verbose and detailed but the spatial bias is retained.
‘The visual field and pathway are important regulators of postural control. Visual input for postural control helps to fixate the position of the head and upper trunk in space, primarily so that the center of mass of the trunk maintains balance over the well-defined limits of foot support…Although postural control is highly dependent upon visual status, higher cortical functions are necessary to differentiate between a fixed person within a moving environment, or a moving person within a fixed environment. Buchanan et al demonstrated how the central nervous system might actively suppress visual information that is inconsistent with afferent postural control input from other sources, such as the somatosensory system…
While vision is an important part of postural control, the information it relays to higher cortical areas remains based on relative perception. Postural corrections initiated by the visual system are made in the direction of visual stimulus. Afferent stimulus provided by the visual field can include either movement of the environment around the person, or movement of the person in the environment…
To further summarize the importance of vision in postural control, Buchanan et al concluded that fixing the head and trunk in space achieves three major functional tasks: 1) it stabilizes the visual field for gaze stabilization, 2) it stabilizes the center of mass of the head and trunk within feet support, and 3) it minimizes the external stress acting upon the head and trunk. Because Buchanan et al showed how visual deprivation destabilizes head and trunk position, this provides evidence that control of the head and trunk is assumed in a top-down mode. This organization may have clinical value when designing treatments to correct abnormal posture.”2
Now that we’ve gotten both a historical and current review of the relationship of vision and posture, let’s shift gears and focus on breaking down that trialogue more.
Maps of Maps
The first thing you need to do when you want to unravel the intricacies of vision and posture is realize we are all experiments of one. When we make assertions about their relationship, it has to be taken with that disclaimer in mind. All we can hope to do is design a good enough map to navigate this mysterious and evolving territory.
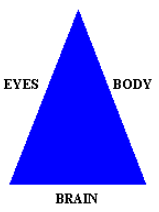
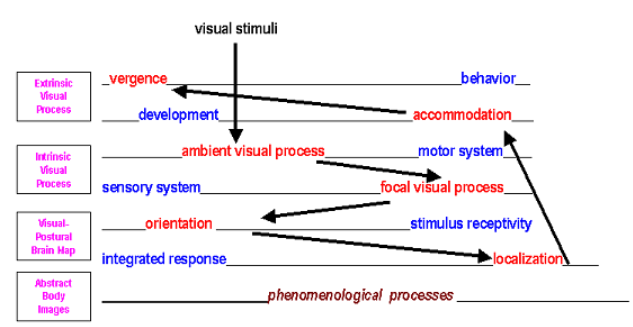
The most basic map we can design this simple, anatomical model below. It put the connection between vision and postural development in a form that allows us to relate it to healing. From this template, we can learn how these three distinct domains interact on a somatic, semantic and systemic level. This is the ‘square one’ we need to be able to access more abstract aspects of an individual and literally step into how they view the world inside-out,which is the core of the somatic paradigm.
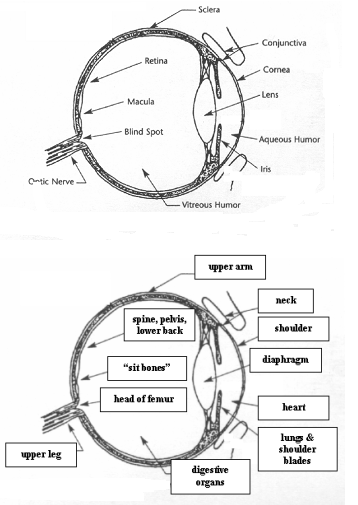
To get that subjective aspect we need to take a decidedly experiential and imaginative detour into the work of Peter Grunwald, a student and teacher of the Bates method and the Alexander technique. Peter has put together some keen insights of the role of vision and the body through his own experience. He has devised a structurally analogous map that correlates various parts of the eye, visual pathways and visual cortex with specific areas of the body. Here’s a list of his findings…
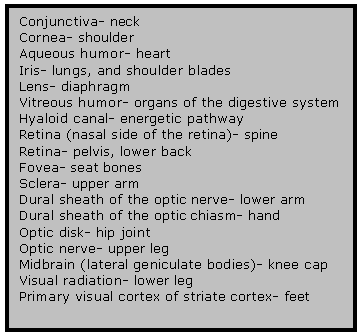
Peter’s method of derivation was particularly of interest here. He incorporated the fundamental links that connect vision and posture by associating the “thought” of a structure within the eye to his bodily response to that “thought”. Peter’s work went on say that inhibiting an unconscious thought which corresponded to a specific area of his eye, and then consciously directing this to a certain area of his eye had an effect on the body. How did the brain monitor that conversation?
The visual cortex takes up a quarter of the entire brain and a full 90% of the brain’s sensory input comes from visual sources. So when an image is processed it impacts the way the eye and body relate functionally by design. Taking a look at the diagrams below, you begin to view the physical eye as a three-dimensional map of the internal structure of the whole body. That coupled with the fact that the eyes are extensions of the brain anyway and you quickly realize how vision and posture, as a composite system, are tied into the regulatory actions of the individual. In that sense, in order to heal, we must learn to “see ourselves” in a whole new light.
~~~~~~~~~~~~~~~~~
The eyes, visual pathways and visual cortex correspond with analogous areas of the body. Specific visual disorders correspond with specific analogous movements and contractions in the body. Suddenly, our literal eye becomes a living map of the figurative body. This opens the door to eavesdropping on the trialogue even more…
Now we can go back to our original map and blend Peter’s awareness into a dynamical model that brings out these distinctions that underlie how the eye, brain and body converse. But before we do that the bridge between the eyes and the spine needs to be crossed. Here’s how. The muscles that control the eye movement arise from the same core of somites that the form the paraspinal muscles. So we get this:
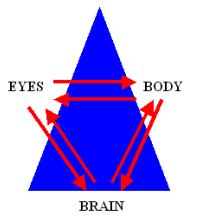
This time we’ve added the component of interaction among the basic three players in this trialogue. Now we can evaluate the clarity of these connections in the context of each individual’s visual limitation as reflected in their postural tone. But we’re still not creating a map we can use to get into the dynamic nature what we’re decoding.
This existential riddle was first encountered by behavioral optometry. They had create their own portable clinical metaphor to better understand how their work addressed the obstacle of making what is subjective a sharable experience. Their “map” spoke of something called the Four Circles and it went like this… One caveat, the four circles of Skeffington are not presented as the model of vision. The four circles is just one among many ways through which one may explain vision.
While attending an optometry conference in the mid-1950’s, A.F. Skeffington, along with his colleagues, were discussing theories about how the visual process unfolded. Through their dinner conversation he arrived at a method to present his ideas graphically. These overlapping circles you see in Figure 6 were the result of a discussion on Boolean logic (just think of a Venn Diagram) and a Ballantine Beer logo...
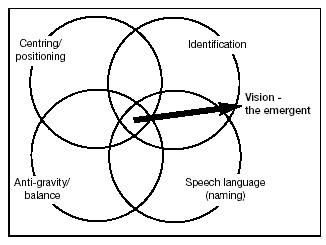
(a three-ringed triangle) he noticed at the time. Neat, huh? What Skeffington did was devise specific questions that each circle represented and then correlated them to the clinical experience. Let’s review his model of explanation here briefly.
The first circle represented ANTI-GRAVITYactivity that related to visual processing. The questions Skeffington attributed to this aspect concerned spatial orientation within and around the body. So the anti-gravity circles answers the basic question of “Where am I?”and that leads to more refined follow-up questions like,“Where am I in space?"and "Where are my body parts in reference to the other parts of me?" which further detail the feedback gained from the initial inquiry. This links the visual process with vestibular activity, bringing top-down and bottom-up processes into one integrated whole body action. This first circle placed vision in a new arena.
The second circle is concerned with CENTERING activity the visual process uses to locate and relate to actual or conceptual objects. It uses the so-called “vergence system”, which includes but is not limited to the ciliary muscles and the extraocular muscles. The centering circle is concerned with efficient ocular motion and will engage body movements that work to square the system off to its focus. To Skeffington’s way of thinking, the centering circle is assigned to answering the question, “Where is it?”, which places it in the role of shifting the focus of the eyes to the target in the inner or outer world. Circle #1 locates “us” and circle #2 finds “them”.
The third circle is designed to work on IDENTIFICATION of the objects the individual encounters by integrating peripheral and central vision to optimize foveal positioning. In Skeffington’s line of reasoning, the identification circle attempts to answer the question, “What is it?”, delineating the figure/ground relationship from the world it perceives. “Current work on magno and parvo cellular pathways of visual control, reviewed by Tychosen, has confirmed this concept.”15 Now, recall that the fovea was analogous to the “sit bones” in our discussion earlier. Can you see how shifts in foveal positioning may impact the tension in the ischiums (sit bones) and vice versa? The reason I stopped to mention this now was that while it may appear that this circle is excluding the body, it is in fact, very aware of the macro-correlation occurring. What happens once this material is organized to use? Let’s add the forth circle to the mix to complete the picture.
The fourth and final circle deals with SPEECH/AUDITORY which allows the individual to name or label the objects in their environment. This allows the nervous system to encode experiences and recall them as needed. In this way the eyes serve as the conduit for our social-conditioning from a very early age. The question that Sheffington assigned to this circle was “What is its name?”which allows us to capture our experiences and encode them semantically. Clinically, it can manifest in both internal and external dialogue. The key to remember here is that Skeffington took the insights from the four circles, distilled it into a useful clinical application, and reframed the way visual limitations are viewed by both himself and the subject.
So now what?
With all these maps it can get very confusing if we don’t keep the ‘big picture’ in mind. Stated simply, the aim is to be able guide both our students, clients or patients and ourselves as educators to a more coherent level of visual-postural integration. When we examine the role common eye conditions have on acuity and other features of the standard parameters of optimal sight, we need to include their impact on the inner lives of the individual as well. To do that, we require an analinear approach to the problem. This combines the analog aspects of felt-sense awareness with the digital or linear models we use to link cause & effect episodically.
To accomplish that, I designed this equation to give both the practitioner and the subject with a set of testable processes to monitor. This is how it breaks down.
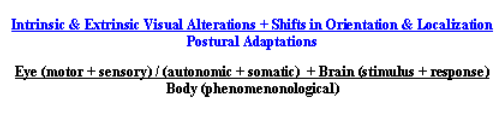
I know it appears complicated. But in reality, the intertwined evolution of the visual and postural dynamic, as a system, no different than other overlapping systems, like circulation and respiration for example. In breaking down any visual disorder developmentally, we must remember to move from the ambient visual processinto the focal visual processto understand the intrinsic aspect of the condition. In this way, motor learning drives sensory integration and promotes visual optimization… our response (localization) is shaped by our receptivity (orientation). Finally, we return to the body from the inside-out, as an experiential template, not a mindless machine. Practitioners must factor in WHO is transforming, not just WHAT is transforming. Keith Holland summed up the essence of vision training in this way.
“The art of arranging conditions so that the patient becomes aware of new relationships in his visual world, and through these new relationships learns to utilize processes that allow him to extract a greater amount of information in a more efficient manner.”
Here’s a schematic to help you appreciate the ‘gravity’ of what Holland proposing.
To go full circle, here’s what Peter Grunwald’s work offers us about a few common visual conditions. If you take away anything from this article, Harmon’s prescient assertion that the priority of vision is to orient us in space. That covers both our inner world and our natural and cultural environment. Most us living in this age of an avalanche of visual stimuli may find it difficult to move our attention within. That’s where the somatic community can fill a much needed role as more young and developing brains are drawn into a world of instant replays, HDTV and social media.
To go full circle, here's what Peter Grunwald's work offers us about a few common visual conditions. If you take away anything from this article, Harmon's prescient assertion that the priority of vision is to orient us in space. That covers both our inner world and our natural and cultural environment. Most us living in this age of an avalanche of visual stimuli may find it difficult to move our attention within. That's where the somatic community can fill a much needed role as more young and developing brains are drawn into a world of instant replays, HDTV and social media.
Myopia and Astigmatism
Myopia this usually develops either in the prenatal development phase, childhood or before the age of 21. It is seldom found later except with extensive near visual tasks ex. computer work or after severe trauma.
Visual aspect
The shortening of the midbrain (lateral geniculate body corresponds to the patella) and spinal cord shortens the optic nerve, which results in overlengthening of the eyeball (torso). Light falls too short of the fovea centralis (coccyx) for clear distant vision and does not sufficiently stimulate the entire retina. Only a fraction of the visual cortex (feet) is used, resulting in reduced function.
Postural aspect
Shortening of the brainstem and spinal cord causes the head to move back and down, shortening the entire body structure (torso corresponds to eyeball). This affects the bone structure of the eye socket in general. One result may be a tilting forwards and down of the lesser wing of the sphenoid bone where the optic nerve (upper leg) reaches from the brain to the eyeball (lower part of the body to the torso). The main feature in myopia is the shortening of the lumbar region (retina) which affects the pelvis, the head of the femur (blind spot) and the femur bone (optic nerve) as well as the patella (lateral geniculate body) and often the feet (visual cortex).
Presbyopia
This is middle aged sight "where the arms are getting too short". It usually begins to affect people after the age of 40 and affects they're near vision.
Visual aspect
It has similar visual shortening as in myopia (even though this may not have affected the person till age 40) with the addition that the ciliary process and particularly the ciliary muscles become inactive through a lack of fine movement. This tops stimulation of the capsule surrounding the lens (diaphragm). When this occurs the lens calcifies and reduces visual accommodation (breathing mechanism affected). This results in lack of sufficient stimulation of the vitreous humor jelly (digestive and reproductive organs) and the aqueous humor (upper chest). The iris (area of lungs and scapula) is also affected.
Postural aspect The bone structure of the shoulder girdle and scapula (cornea) seems affected, as in the rotation of the upper arms (sclera). This shows mostly as a slumping in the chest area (lower front area of the eye) and narrowing in the upper back (upper front area of the eye). And as this occurs mostly with the postural patterns of myopia add the myopic movement pattern to get the full picture throughout the body.
Stabismus This may develop at prenatal developmental stages, during birth (forceps delivery or a quick birth, where the occiput was not fully released) or during developmental stages, particularly during crawling. It is often found alongside hyperopia or myopia.
Visual aspect
On or both eyes turn inwards or outwards. Visual cortex (feet) dysfunction, affecting specifically the optic nerve (upper leg) and blind spot (head of the femur).
Postural aspect
The side of the body with the eye turn is affected primarily by rotation of the upper leg (optic nerve) inwards. The lesser wing of the sphenoid bone is rotated forwards and down, affecting the pathway for the optic nerve. More often than not the child missed the cross-crawling stage of development.
For further reading…
1 History Of Behavioral Optometry
2 Reflex Control Of The Spine & Posture
There’s obviously much more to this story. I’d like to invite you to visit my latest application of these principles and explore some of my contributions to this topic.

Thank you for this time in your space…
Dr. Mark Filippi
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
For more resources to naturally improve your vision visit Dr. Grossman's new site!